The NVR is commissioned by the Healthcare Quality Improvement Partnership (HQIP) as part of the National Clinical Audit and Patient Outcomes Programme and is designed to promote quality improvement within NHS hospitals performing vascular surgery by providing information on their performance. In this summary we present data with direct relevance to vascular anaesthetists. The full report is available at 2025 NVR State of the Nation Report - VSQIP - Vascular Services Quality Improvement Programme
The NVR 2025 report highlights a decline in carotid endarterectomy annual volumes, with a 53% adherence rate to the 14-day symptom-to-surgery target. Elective infra-renal AAA repairs showed a 62% endovascular rate, though meeting the 8-week repair target remains challenging. The report highlights higher mortality in complex open (9.9%) versus complex endovascular (1.5%) AAA repairs, and a sharp contrast between elective (1.8%) and non-elective (14.2%) revision procedures.
Carotid Endarterectomy
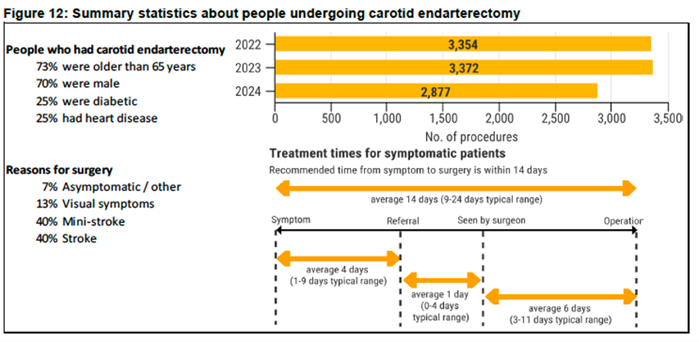
In 2024, 2,877 carotid endarterectomies were carried out in the UK, down from 3,324 in 2023, representing an estimated case ascertainment rate of 87%.
Procedure volumes have declined markedly since 2011, when nearly 6,000 operations were performed. A summary of case volumes and patient characteristic are shown in Figure 12 below.
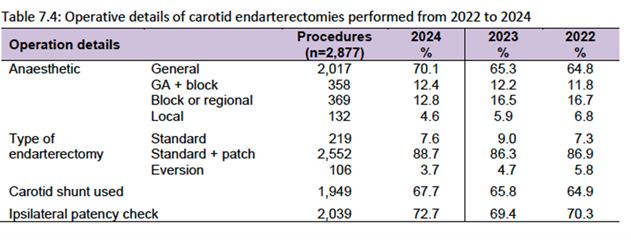
Anaesthetic Type and Operative Details
Table 7.4 shows the operative details of unilateral carotid endarterectomies performed from 2022 to 2024.
There were 2,719 patients (94.5%) with symptomatic disease.
- TIA was the most common symptom (42.5%), followed by stroke (42%).
- 70.4% of patients had at least 70% stenosis in their ipsilateral carotid artery at the time of operation.
Treatment Pathways
The NICE target time from symptom to operation is 14 days in order to minimise the chance of a high-risk patient developing a stroke.
In 2024, the median interval from symptom onset to surgery for patients undergoing CEA was 14 days (IQR 9-24), with 53% treated within this time frame. This represents a modest improvement compared with 2023, when the median was also 14 days but only 49% of patients received treatment within 14 days.
For the three distinct phases within this pathway, the median time delays in 2024 were:
- 4 days (IQR 1-9) from symptom to first medical referral
- 1 day (IQR 0-4) from first medical referral to being seen by the vascular team, and
- 6 days (IQR 3-11) from being seen by the vascular team to undergoing CEA.
Before the pandemic, in 2019, 56% of patients were treated within 14 days. However, median waiting times exceeded 20 days in eleven NHS trust organisations, which is more than in 2023. The reasons for these longer delays warrant further investigation at a local level.
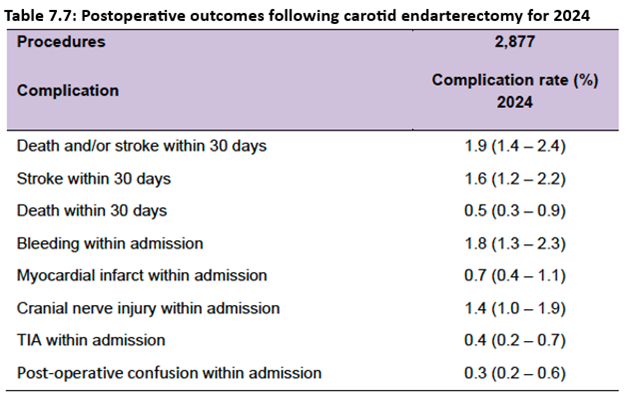
Outcomes After Carotid Endarterectomy
Complication rates for the 2,877 procedures performed in NHS hospitals in 2024 are presented in Table 7.7. Rates for individual complications ranged from approximately 0.3% to 1.9% and have remained broadly stable across recent NVR Annual Reports.
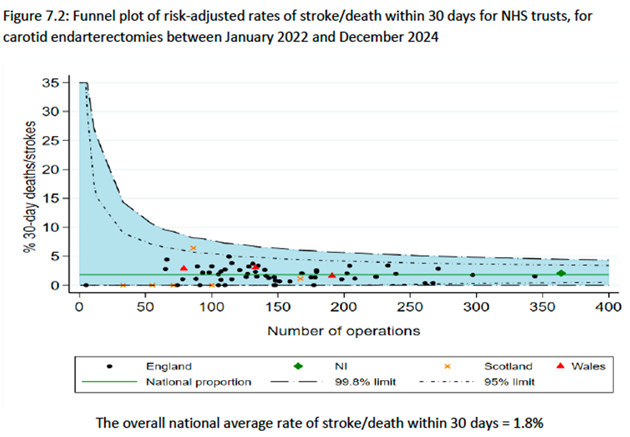
The primary measure of safety after carotid endarterectomy is the rate of death or stroke within 30 days of the procedure. The risk-adjusted values for each NHS trust for this outcome indicator are shown in Figure 7.2. Between 2022 and 2024, all NHS organisations were within the expected distance of the overall national average rate of 1.8% (i.e., they were within the 99.8% control limits).
Recommendations:
- Ensure timely referral and expedited surgery for patients with symptomatic carotid disease with measures to reduce waiting times to carotid endarterectomy.
- The target time from symptom to operation is 14 days in order to minimise the chance of a high-risk patient developing a stroke.
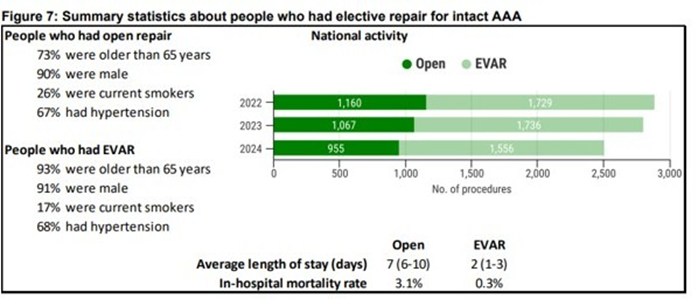
Elective Infra-renal AAA
The NVR received information on 2,511 people who had an elective repair of an unruptured infra-renal AAA in 2024, which corresponds to an estimated case-ascertainment rate for the UK of 91% (for England = 91%; for Wales = >100%; for Scotland = 64%; for NI = 100%).
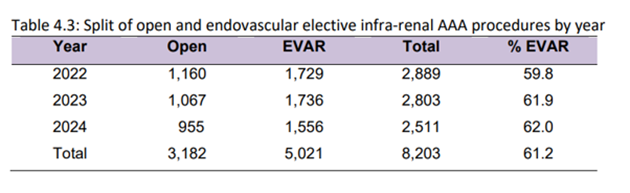
Of these, 62.0% of procedures were endovascular repair (EVAR) and 38.0% were open repair (Figure 7). This split between EVAR and open repair varied across NHS organisations – among the 59 NHS vascular units that performed elective AAA repair in 2024, 10 units performed EVAR in over 80% of procedures, while 7 units performed EVAR in less than 40% of cases.
Time from vascular assessment to elective repair for people with intact AAA
Overall, 33% of patients with AAA had their procedure within 8 weeks (compared with 31% in 2023). At two units, a quarter of people waited more than 220 days for their procedure in 2024 (Figure 8). The National AAA Screening Programme (NAAASP) has defined a standard of 8 weeks from the date of referral from the NAAASP to the date of repair. The NAAASP recommends that NHS organisations should meet this standard for at least 80% of patients. Meeting this standard remains a challenge for the 59 NHS vascular units performing elective repairs in 2024, and the median time from assessment to procedure was 81 days. Most people who had an elective infrarenal AAA repair in 2024 received care consistent with the standards in the Vascular Society AAA Quality Improvement Framework.
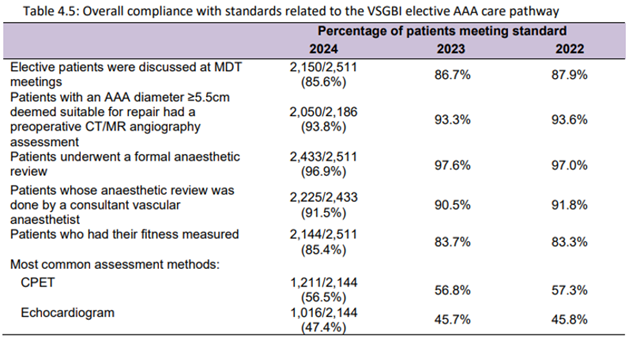
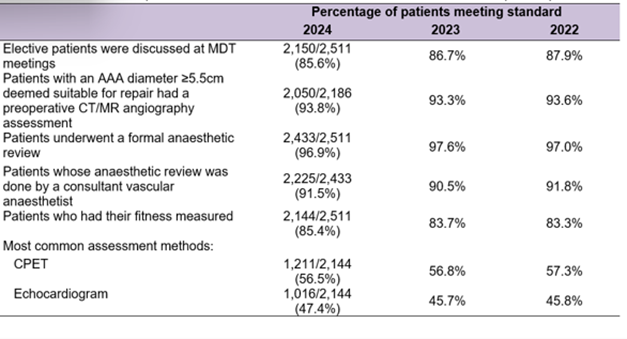
Preoperative pathway for elective infra-renal AAA
Outcomes after elective infra-renal AAA repair
Between January 2022 and December 2024, the risk-adjusted in-hospital mortality rates for all NHS vascular units were within the expected range, as defined by the national average of 1.3%.
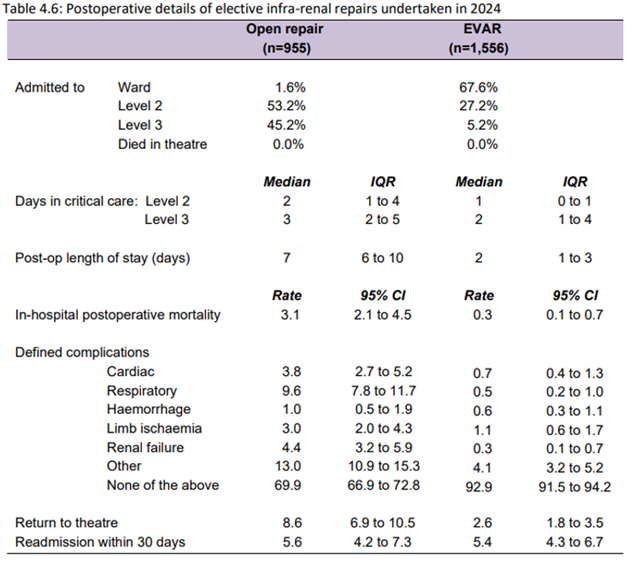
Table 4.5: Overall compliance with standards related to the VSGBI elective AAA care pathway
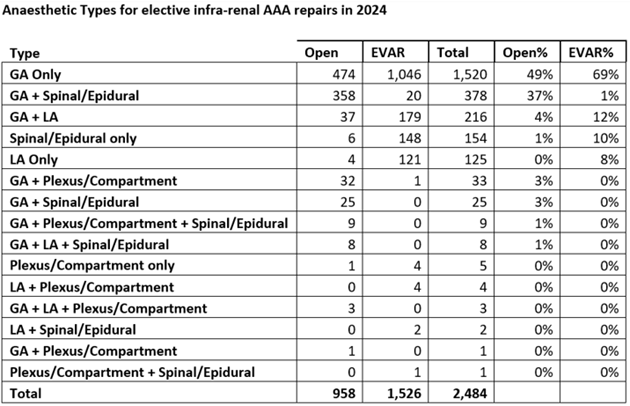
Anaesthetic Choices for elective AAA repair
Complex Aneurysm Repair
The most common procedures are Fenestrated EVAR (FEVAR) and Branched EVAR (BEVAR), which are performed when the aortic aneurysm is close to or involves other arteries branching from the aorta.
In 2022-24, there were 1,532 endovascular procedures (which included 1,216 FEVAR and 290 BEVAR procedures) and 253 complex open repair procedures. The majority of the procedures were performed in men (86%). Over 80% were current or ex-smokers.
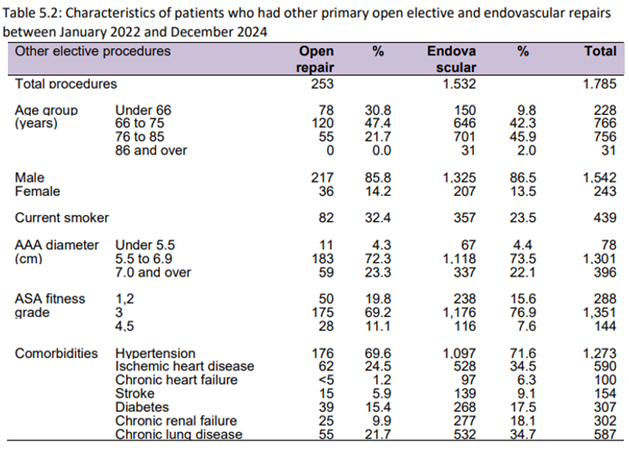
KEY MESSAGES: Postoperative mortality rates were lower after complex endovascular repairs (1.5%) than after complex open repairs (9.9%). Rates of readmission within 30 days were 9.7% for open procedures and 7.3% for endovascular procedures.

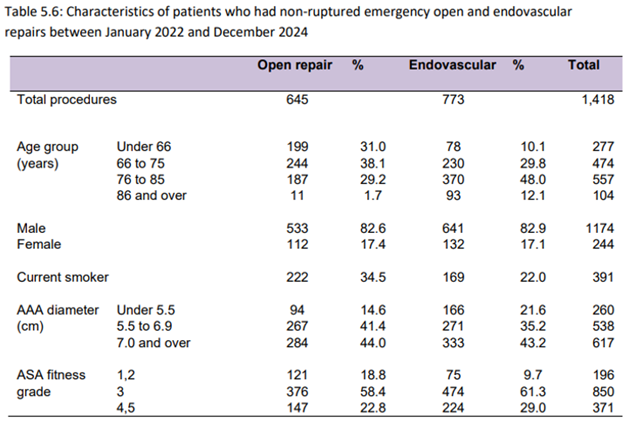
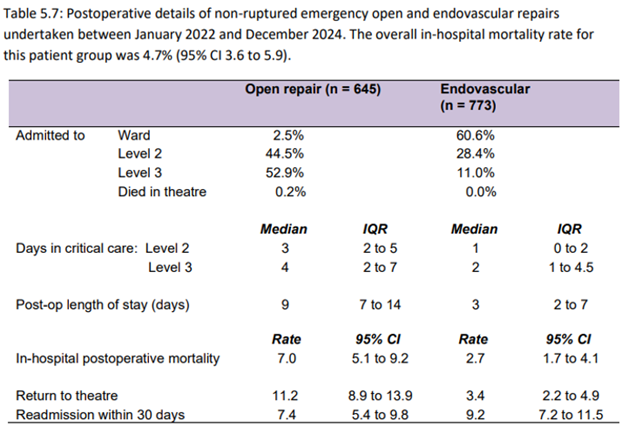
URGENT UNRUPTURED AORTIC ANEURYSM PROCEDURES
Some people have their intact AAA repaired after being admitted as an emergency admission (or are recorded as having an emergency operative procedure after an elective admission). Between 2022 and 2024, the NVR received details of 1,418 such cases.
These patients tend to have larger aneurysms [6.5 cm (5.6 – 8.0) for any unruptured emergency admission] and have worse outcomes as they tend not to have had the pre-operative work-up, when compared to electively admitted AAA repairs. Postoperative mortality rates were 2.7% for endovascular repairs and 7.0% for open repairs.
REVISION AORTIC PROCEDURES
Since 2020 the NVR has collected information on different types of revision procedures that may be required after an initial primary aortic repair procedure (open and endovascular). These procedures are undertaken to address disease progression or complications from the original procedure, and they represent a growing component of vascular unit activity. Between 2022-2024, the NVR received information about 726 elective revision procedures and 373 non-elective revisions.
Common elements of these procedures (more than one element can be undertaken) in each revision included:
- Removal (explant) of a previously inserted graft: 73 elective; 59 non-elective
- Insertion of a new stent graft within / alongside the existing graft (relining): 199 elective; 160 non-elective
- Insertion of a new stent graft to extend the repair into the iliac arteries (distal extension): 243 elective; 94 non-elective
- Embolisation for an endoleak complication after an EVAR procedure: 151 elective; 42 non-elective
Postoperative mortality rates for elective and non-elective revision AAA procedures were 1.8% and 14.2%, respectively.
Repair of Thoracic Aortic Conditions
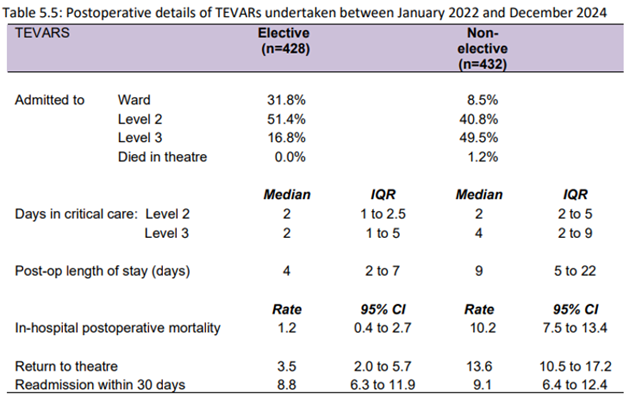
People who suffer from a thoracic aortic aneurysm or aortic dissection are increasingly treated using a thoracic endovascular aortic repair (TEVAR). This procedure is performed in either a cardiothoracic unit or specialist vascular unit. People may present as an emergency admission and have a TEVAR with minimal delay; in some people, the condition may be without symptoms and may be safely treated electively. In 2022-24, there were 432 emergency and 428 elective TEVAR procedures performed by 41 UK vascular units (Figure 10).
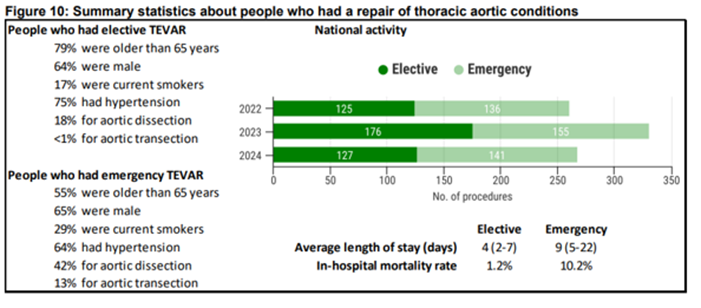
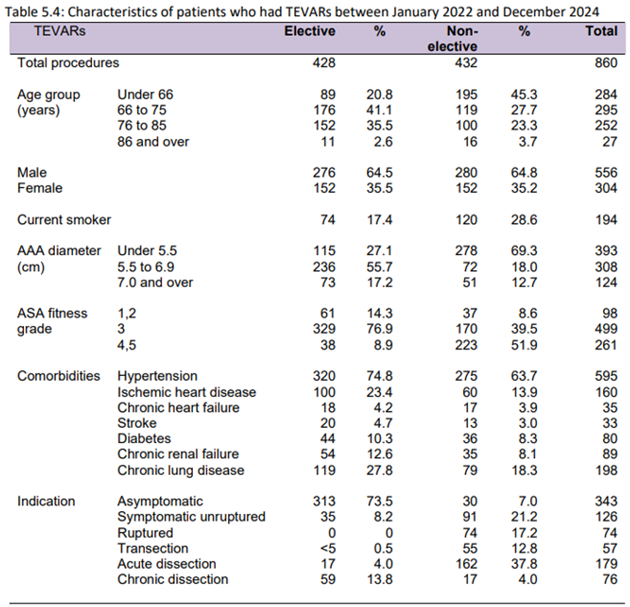
In 2022-24, in-hospital postoperative mortality rates after TEVAR were 10.2% for emergency and 1.2% for elective procedures performed by UK vascular units. Rates of readmission within 30 days were 8.8% for elective procedures and 9.1% for emergency procedures.
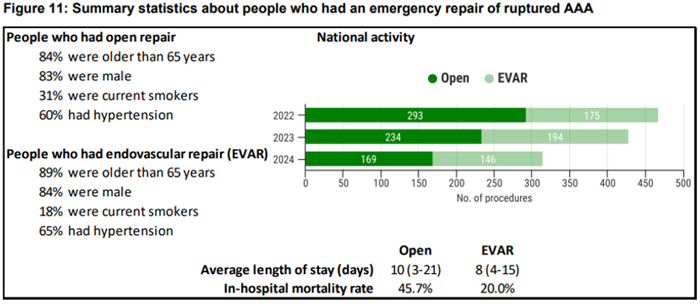
Ruptured AAA
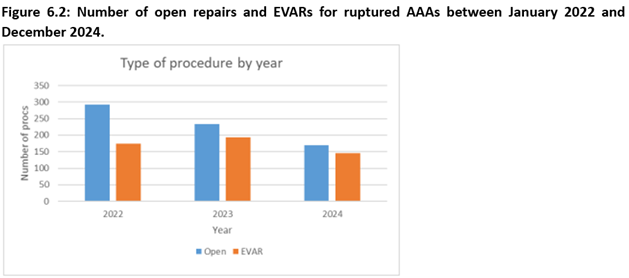
The NVR recorded 1,211 emergency repairs of a ruptured abdominal aneurysm between January 2022 and December 2024, with a fall from year to year (Figure 11). The numbers have decreased significantly since 2015 when over 900 repairs were performed, compared to 315 in 2024. Estimated case ascertainment in 2022-2024 was 94% (for England = 92%; for Wales = >100%; for Scotland = 73%; for NI = 100%).
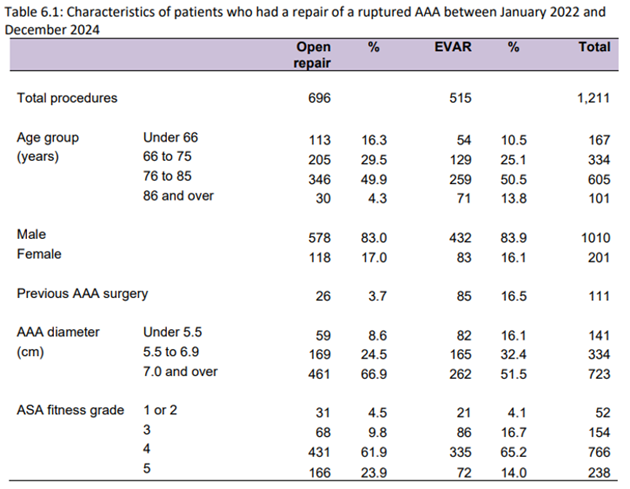
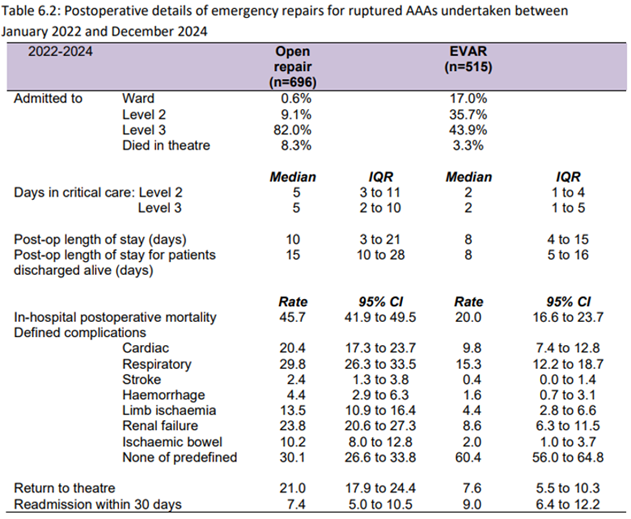
KEY MESSAGES: In 2024, 46% of people with ruptured AAA had an EVAR procedure. Between 2022 and 2024, there was variation across units in the proportion of procedures performed as EVAR, with around a third of units performed more EVARs than open repairs for ruptured AAA. There may be potential in expanding the use of EVAR for ruptured AAA. For people with rAAA treated in 2022-2024, the in-hospital postoperative mortality rates for EVAR and open repairs were 20.0% and 45.7%, respectively. We caution against comparing these mortality figures for EVAR and open repair because people who have open procedures may represent the more complex cases that are unsuitable for endovascular repair. Rates of readmission within 30 days were 7.4% for open repair and 9.0% for EVAR. During the three-year period 2022-2024, all NHS organisations had in-hospital postoperative mortality rates within the expected range after repair for ruptured AAA. The overall national average mortality rate for this period was 34.8%
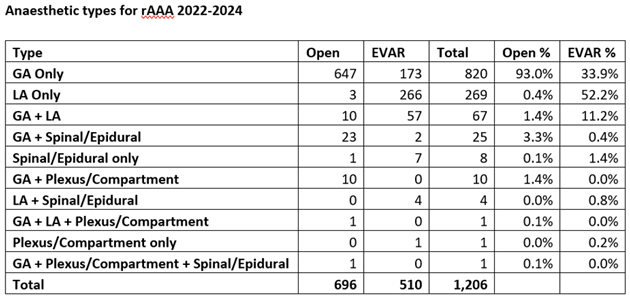
Anaesthetic Choices for ruptured AAA repair
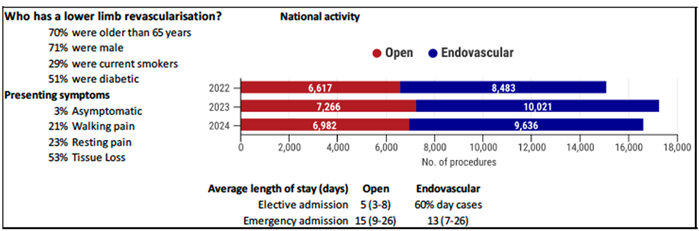
Lower Limb Revascularisation
In 2024, more than 16,618 revascularisation procedures for chronic limb-threatening ischaemia (CLTI)—including endovascular, hybrid, and open bypass—were performed, compared with 14,000 in 2022.
During 2024:
- 6,982 bypass or open procedures were recorded (4,089 elective and 2,893 non-elective), of which 2,453 were hybrid revascularisations.
- 9,636 endovascular procedures were undertaken (6,015 elective and 3,621 non-elective).
The proportion of hybrid procedures has increased in recent years, accounting for 14.8% of all lower limb revascularisations in the UK, up from 9.9% in 2020. Estimated case ascertainment rates in 2024 were 89% for bypass procedures and 58% for angioplasty.
A summary of patient and operative details is shown below.
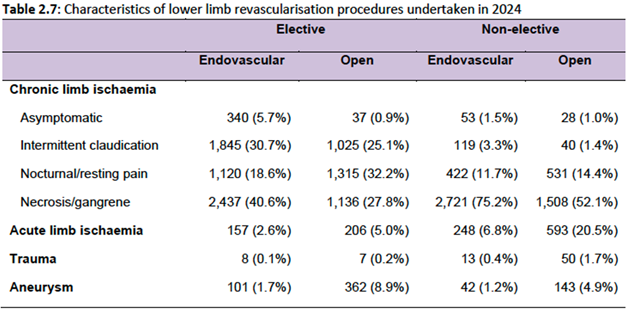
Among patients undergoing open surgical procedures, the majority were aged over 70 years, accounting for 49.1% of elective and 51.8% of non-elective cases. Most patients had coexisting conditions, with hypertension being the most prevalent (69.1% elective, 64.6% non-elective), followed by diabetes (37.5% elective, 43.1% non-elective) and ischaemic heart disease (29.4% elective, 31.2% non-elective). A minority had no recorded co-morbidities (10.8% elective, 11.6% non-elective).
In terms of medical therapy, 85% of elective patients and 75.2% of non-elective patients were documented as receiving a single antiplatelet agent. Statin use was also high, recorded in 83.1% of elective patients and 75.5% of non-elective patients.
Most endovascular procedures in 2024 (88.1%) were performed under local anaesthetic, with 3.0% under regional and 8.9% under general anaesthetic. For open procedures in 2024, 89.8% were performed under general anaesthetic, 7.7% under regional and 2.5% under local.
The following table (2.7) shows the characteristics of lower limb revascularisation procedures undertaken in 2024.
In 2024, 5,182 patients with chronic limb-threatening ischaemia (CLTI) were admitted non-electively, an increase from 4,624 in 2022. The median time from admission to intervention was 6 days (IQR 3–9).
The proportion of patients undergoing revascularisation within 5 days was 49% in 2024, compared with 50.3% in 2023, 51.1% in 2022, and 53.9% in 2021, indicating a gradual decline. Among the 60 NHS organisations performing at least 10 non-elective CLTI procedures:
- 27 units had at least 50% of patients waiting more than 5 days
- 18 units had at least 25% of patients waiting more than 10 days
- 18 units achieved revascularisation within 5 days for more than half of their patients
A total of 4,089 open elective procedures (58.6%) and 2,893 open non-elective procedures (41.4%) were performed in 2024. Most open procedures (93.9%) took place between 8am and 6pm on weekdays, including 98.7% of elective and 87% of non-elective cases. At least 75% of open surgical procedures were carried out on planned lists in all but two NHS trusts submitting 10 or more cases to the NVR (63/65 trusts; 96.9%).
Overall, the proportion of patients treated within 5 days of admission declined slightly from 53% in 2023 to 51.9% in 2024. Median time to revascularisation remained at 5 days (IQR 2–8) in 2024, consistent with 2023 and 2022 (both 5 days, IQR 3–9), but longer than in 2020 (4 days, IQR 2–8).
The median length of stay for open procedures was 5 days (IQR 3–8) for elective cases and 15 days (IQR 9–26) for non-elective cases.
Complications were relatively uncommon: 85.5% for elective and 72.1% for non-elective procedures, however, those undergoing non-elective procedures had a generally higher complications rate and re-intervention rates than those undergoing elective procedures, with limb ischaemia (7.7% non-elective, 2.3% elective), and respiratory (3.9% non-elective and 2.2% elective) complications being the highest. Table 2.9 shows the postoperative outcomes after lower limb revascularisation for 2024 by procedure type.
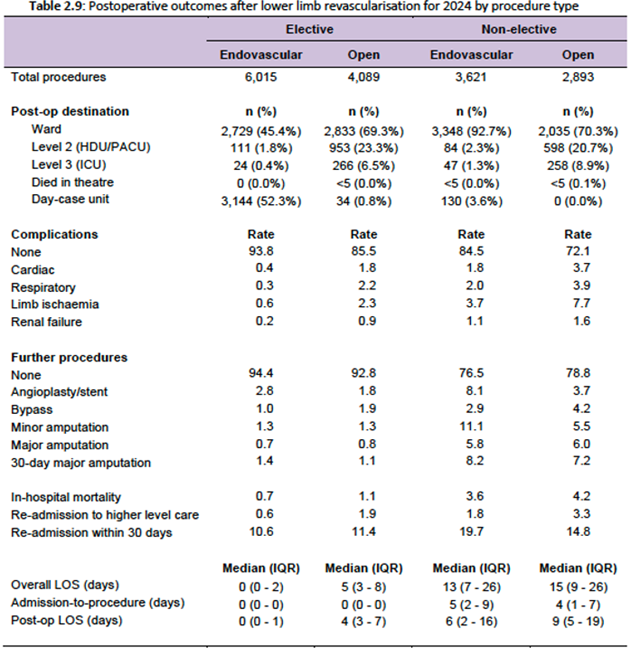
The re-intervention rate (angioplasty/stent, bypass, minor and major amputation, 30-day amputation) was 6.9% for elective procedures and 26.6% for non-elective procedures. This was lower from 2022, where the re-intervention rate was 7.5% for elective procedures and 28% for non-elective procedures.
The In-hospital postoperative mortality rate was 1.1% for elective patients and 4.2% for non-elective patients. All NHS Trusts had a risk-adjusted rate mortality that fell within the expected range of the overall national average of 1.6% (95% CI: 1.5%-1.8%).
Recommendations:
- Patients admitted with non-electively with chronic limb ischaemia should have a revascularisation procedure within 5 days.
- Improved data entry for this group especially for those who require a second unplanned procedure during the same admission.
- Trusts should aim to perform at least 75% of lower limb revascularisation on planned operating lists.
Lower Limb Amputation
This chapter outlines patterns of care and clinical outcomes for patients undergoing unilateral major lower limb amputation for vascular disease during the audit period from January to December 2024.
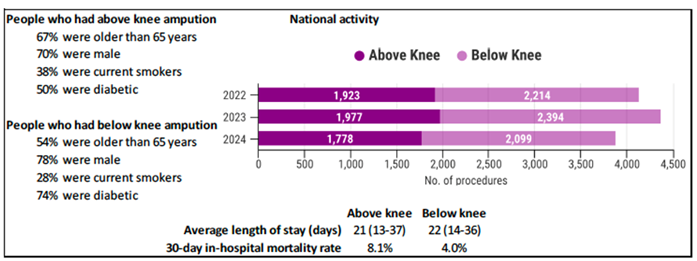
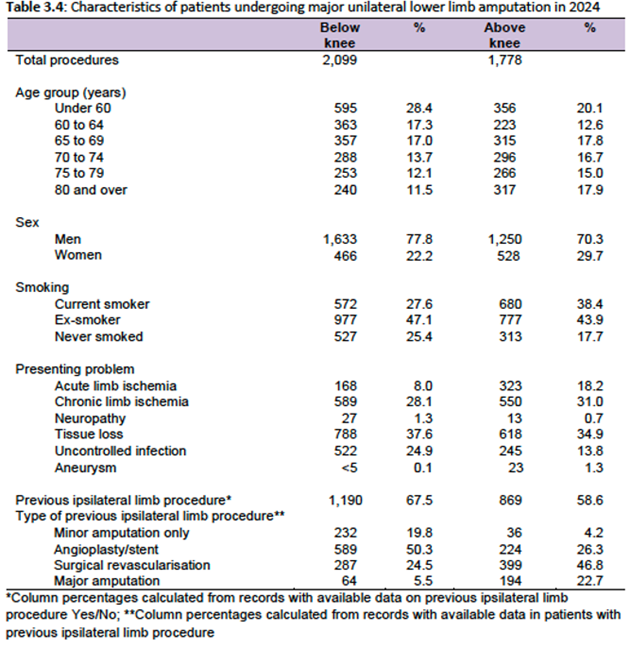
During this period, 3,877 primary major unilateral amputations were recorded in the NVR, comprising 1,778 (45.9%) above-knee amputations (AKAs) and 2,099 (54.1%) below-knee amputations (BKAs), yielding an overall AKA:BKA ratio of 0.85 (95% CI: 0.80-0.90). Vascular units are expected to maintain an AKA:BKA ratio below 1, and most NHS vascular units fell within this target range (39 out of 56), whilst 17 units had a ratio above one and four units had a ratio above two.
Future research should examine the factors associated with higher ratios and inform the development of targeted interventions to reduce them. Improving outcomes for patients undergoing major lower limb amputation has been identified as a key research priority by both vascular patients and clinicians.
A summary of patient characteristics is shown below.
Most patients had at least one co-morbidity. Polypharmacy was common, with frequent use of antiplatelet agents, statins, antibiotics, and thromboprophylaxis.
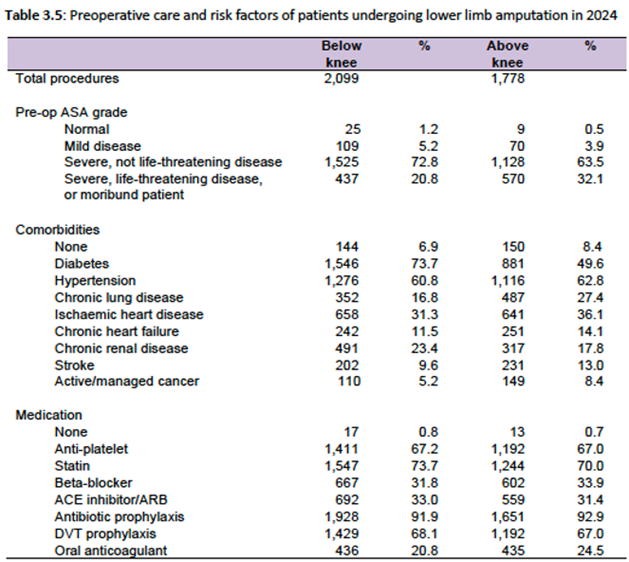
Table 3.4 summarises the characteristics of patients undergoing lower limb amputation in 2024, while Table 3.5 presents the pre-operative risk factors for this cohort.
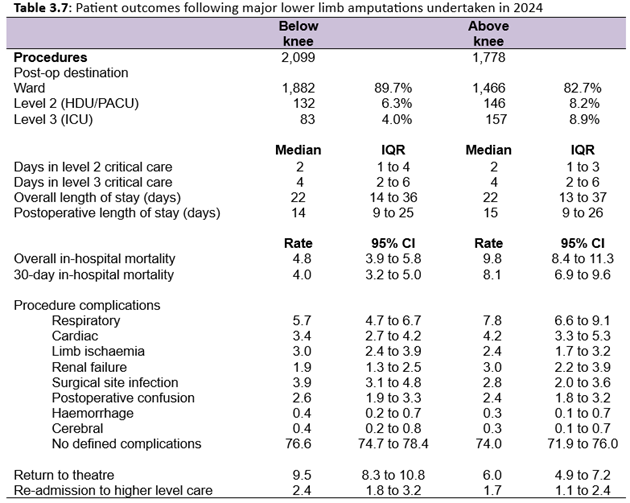
Outcomes After Major Amputation
Patient outcomes immediately following a major lower limb amputation is summarised in table 3.6. It is recommended that major amputations should be undertaken on a planned operating list during normal working hours, and a consultant surgeon should operate or at least be present in the theatre to supervise. In 2024, over 90% of major amputations (BKAs and AKAs) were performed during the day (8am to 6pm), and a consultant surgeon was reported as present for three-quarters of the procedures. In the 55 NHS vascular units with at least 10 procedures in 2024, 34 units reported a consultant was present in theatre for over 80% of procedures.
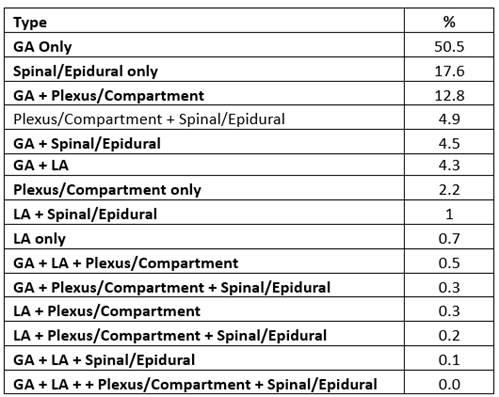
Anaesthetic Choice for Amputation
Key Messages
The overall rate of 30-day in-hospital death for major lower limb amputations in 2024 was 5.9%. As expected, it was higher for AKA (8.1%) than BKA (4.0%).
All NHS organisations had an adjusted 30-day in-hospital mortality rate that fell within the expected range of the overall 30-day in hospital mortality rate (national average = 5.9% for 3 years from 2022 to 2024).
Rates of readmission within 30 days were 10.4% for AKAs and 11.6% for BKAs.